Medical Questionnaire
Save, fill-In The Blanks, Print, Done!

Download Medical Questionnaire
Adobe Acrobat (.pdf)- This Document Has Been Certified by a Professional
- 100% customizable
- This is a digital download (63.38 kB)
- Language: English
- We recommend downloading this file onto your computer.

How to write a Medical Questionnaire? Download this Medical Questionnaire template that will perfectly suit your needs.
Our collection of online health templates aims to make life easier for you. Our site is updated every day with new health and healthcare templates. By providing you this health Medical Questionnaire template, we hope you can save precious time, cost and efforts and it will help you to reach the next level of success in your life, studies or work!
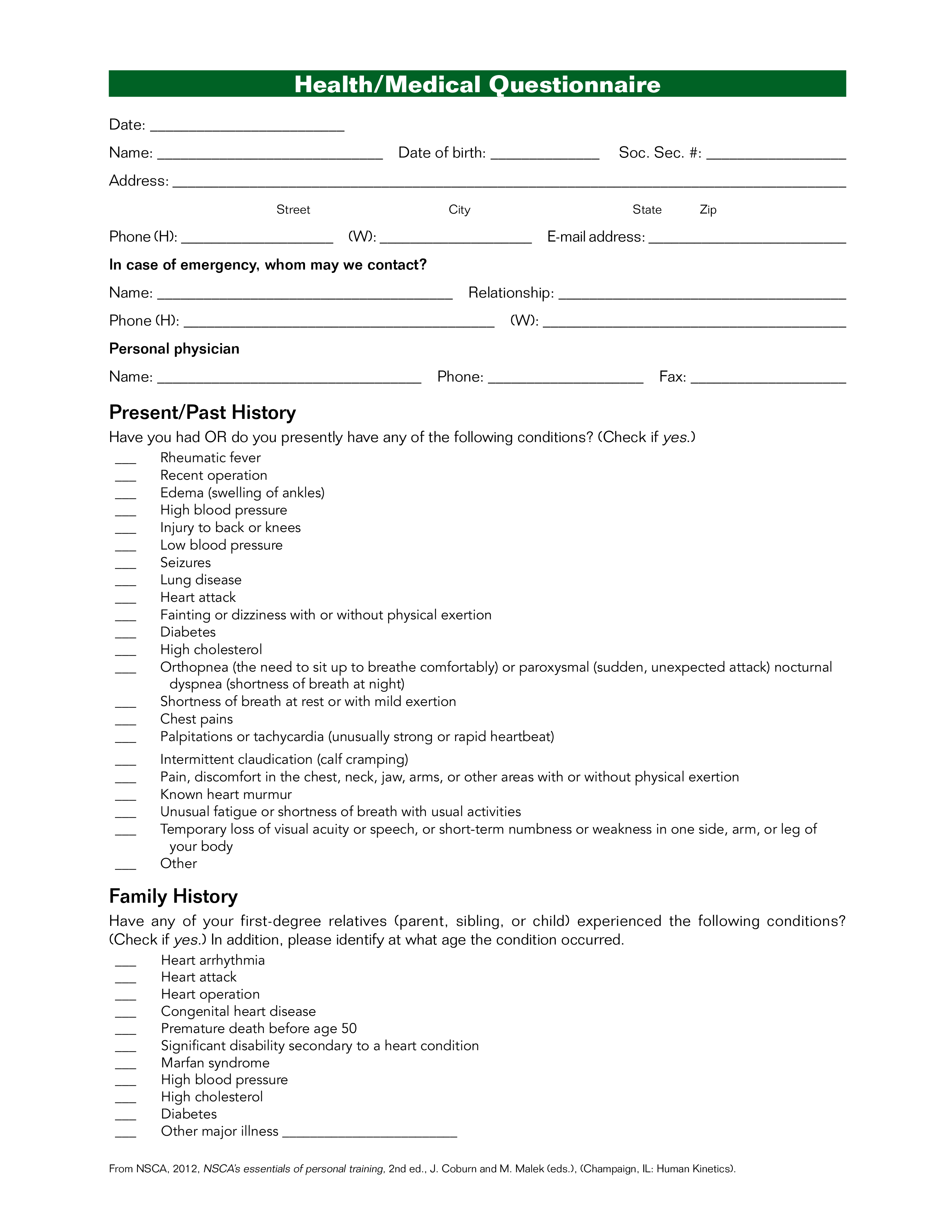
: __________________ Address: _______________________________________________________________________________________ Street City State Zip Phone (H): ____________________ (W): ____________________ E-mail address: __________________________ In case of emergency, whom may we contact Name: ______________________________________ Relationship: _____________________________________ Phone (H): ________________________________________ (W): _______________________________________ Personal physician Name: __________________________________ Phone: ____________________ Fax: ____________________ Present/Past History Have you had OR do you presently have any of the following conditions (Check if yes.) ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ Rheumatic fever Recent operation Edema (swelling of ankles) High blood pressure Injury to back or knees Low blood pressure Seizures Lung disease Heart attack Fainting or dizziness with or without physical exertion Diabetes High cholesterol Orthopnea (the need to sit up to breathe comfortably) or paroxysmal (sudden, unexpected attack) nocturnal dyspnea (shortness of breath at night) Shortness of breath at rest or with mild exertion Chest pains Palpitations or tachycardia (unusually strong or rapid heartbeat) Intermittent claudication (calf cramping) Pain, discomfort in the chest, neck, jaw, arms, or other areas with or without physical exertion Known heart murmur Unusual fatigue or shortness of breath with usual activities Temporary loss of visual acuity or speech, or short-term numbness or weakness in one side, arm, or leg of your body Other Family History Have any of your first-degree relatives (parent, sibling, or child) experienced the following conditions (Check if yes.) In addition, please identify at what age the condition occurred..
This Medical Questionnaire is intuitive, ready-to-use and structured in a smart way. Try it now and let this Medical Questionnaire sample inspire you.
We certainly encourage you to download this Medical Questionnaire now and use it to your advantage!
Also interested in other health and healthcare templates? AllBusinessTemplates is the most elaborate platform for downloading health templates and is updated every day with new health and healthcare related templates! Just search via our search bar or browse through our thousands of free and premium health forms and templates, contract, documents, letters, which are used by professionals in the healthcare industry. For example health care directive, mental health treatment plan, health management report, allergy log, healthy weekly meal plans, sick leave letter, health evaluation form, and much more...
DISCLAIMER
Nothing on this site shall be considered legal advice and no attorney-client relationship is established.
Leave a Reply. If you have any questions or remarks, feel free to post them below.