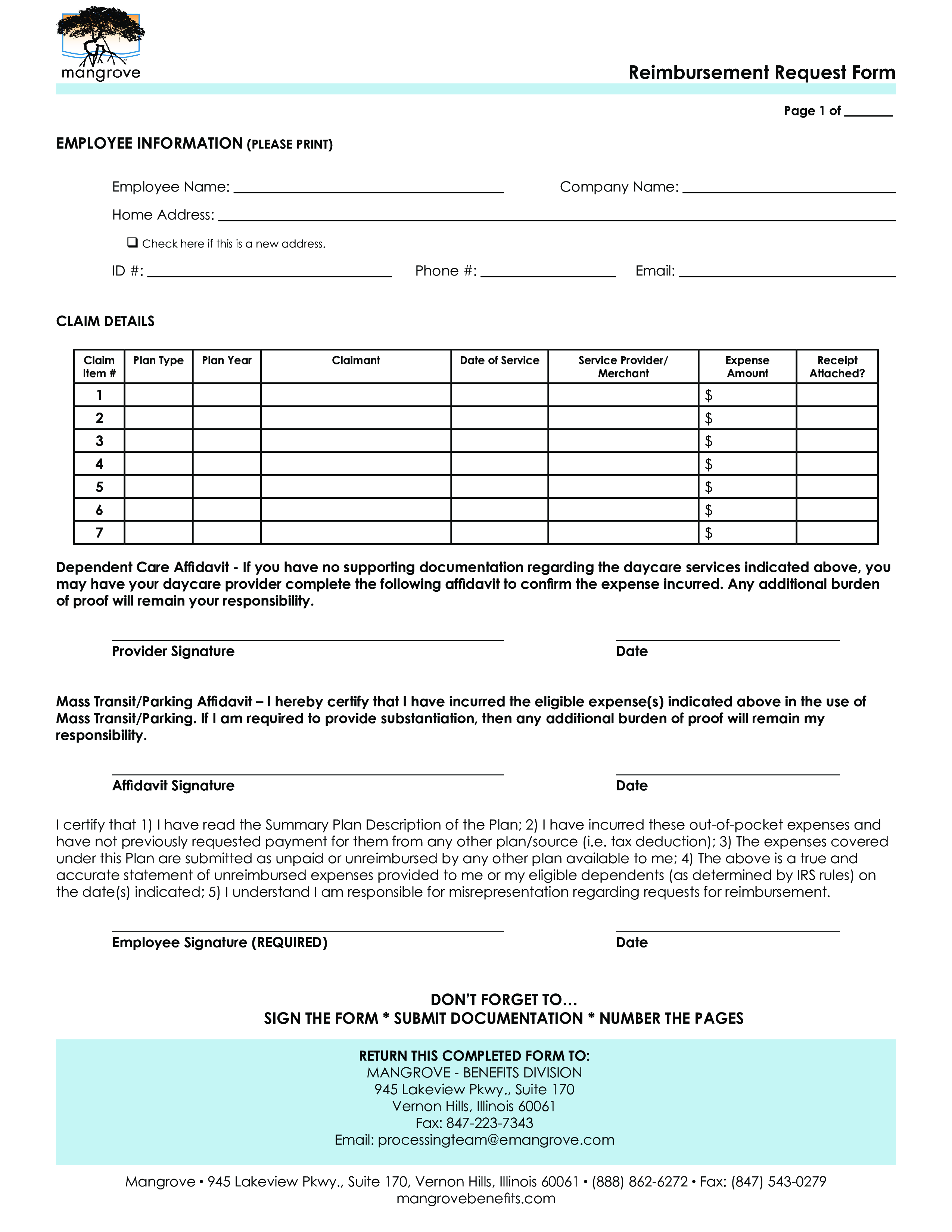
Reimbursement Request Form
Save, fill-In The Blanks, Print, Done!

Download Reimbursement Request Form
Adobe Acrobat (.pdf)- This Document Has Been Certified by a Professional
- 100% customizable
- This is a digital download (166.35 kB)
- Language: English
- We recommend downloading this file onto your computer.

Are you looking for a professional Reimbursement Request Form? If you've been feeling stuck or lack motivation, download this template now!
This Reimbursement Request Form template can help you find inspiration and motivation and covers the most important topics that you are looking for and will help you to structure and communicate in a professional manner with those involved.
DO NOT RETURN THIS INSTRUCTION PAGE WITH YOUR REIMBURSEMENT FORM RETURN THIS • Please enter the requested information for your claim to be considered for reimbursement.
• Each claim item should be entered, itemized per receipt or documentation, in the same order you are enclosing
the documents.
• PLEASE NUMBER THE TOP OF THE FOLLOWING PAGE(S) WITH THE CLAIM ITEM #.
• Provide legible supporting documentation from an independent 3rd party for your claim (i.e. receipt, doctor’s bill,
or Explanation of Benefits (EOB)), which must include:
o Date of service or sale date of the eligible product (must match claim details entry below)
o Name of person or organization that provided the service or product
o Type of service provided or description of eligible product
o Amount of expense (the portion you are responsible for paying)
• Sign and date the Request Form. Forms without a signature will not be accepted or processed.
HELPFUL HINTS
• Do - Keep documentation in order (e.g. number the top of the page with the claim line item #), circle
applicable items on the documentation enclosed, tape small receipts to a full sheet of paper, use as many sheets
for additional expenses, indicate whether you or your dependent incurred the expense under
“Claimant.”
• Do Not - Include credit card receipts/statements or canceled checks, highlight any part of the documentation,
staple multiple receipts to the form or sheet of paper, mail the same form after you faxed or emailed it.
• Reference the following Plan Type - F = Health FSA, D = Dependent Care FSA, H = HRA, P = Parking, T = Transit
• If you are submitting an HRA expense, make sure you are aware of the HRA Plan Design and any requirements of
the type of documentation we need in order to process your claim (i.e. if you’re only reimbursed for
deductible expenses, the documentation provided must indicate the expense was applied towards
deductible).
Feel free to download this intuitive template that is available in several kinds of formats, or try any other of our basic or advanced templates, forms, or documents. Don't reinvent the wheel every time you start something new...
Download this Reimbursement Request Form template and save yourself time and effort! You will see completing your task has never been simpler!
DISCLAIMER
Nothing on this site shall be considered legal advice and no attorney-client relationship is established.
Leave a Reply. If you have any questions or remarks, feel free to post them below.
Related templates
Latest templates
Latest topics
- Google Docs Templates
How to create documents in Google Docs? We provide Google Docs compatible template and these are the reasons why it's useful to work with Google Docs... - IT Security Standards Kit
What are IT Security Standards? Check out our collection of this newly updated IT Security Kit Standard templates, including policies, controls, processes, checklists, procedures and other documents. - Letter Format
How to format a letter? Here is a brief overview of common letter formats and templates in USA and UK and get inspirited immediately! - Google Sheets Templates
How to work with Google Sheets templates? Where to download useful Google Sheets templates? Check out our samples here. - Influencer Marketing Templates
What makes a good influencer? Check out our effective and useful Influencer Marketing Templates here!
cheese