Sample Product Repair Order Form 1
Save, fill-In The Blanks, Print, Done!

Download Sample Product Repair Order Form 1
Adobe Acrobat (.pdf)- This Document Has Been Certified by a Professional
- 100% customizable
- This is a digital download (134.02 kB)
- Language: English
- We recommend downloading this file onto your computer.

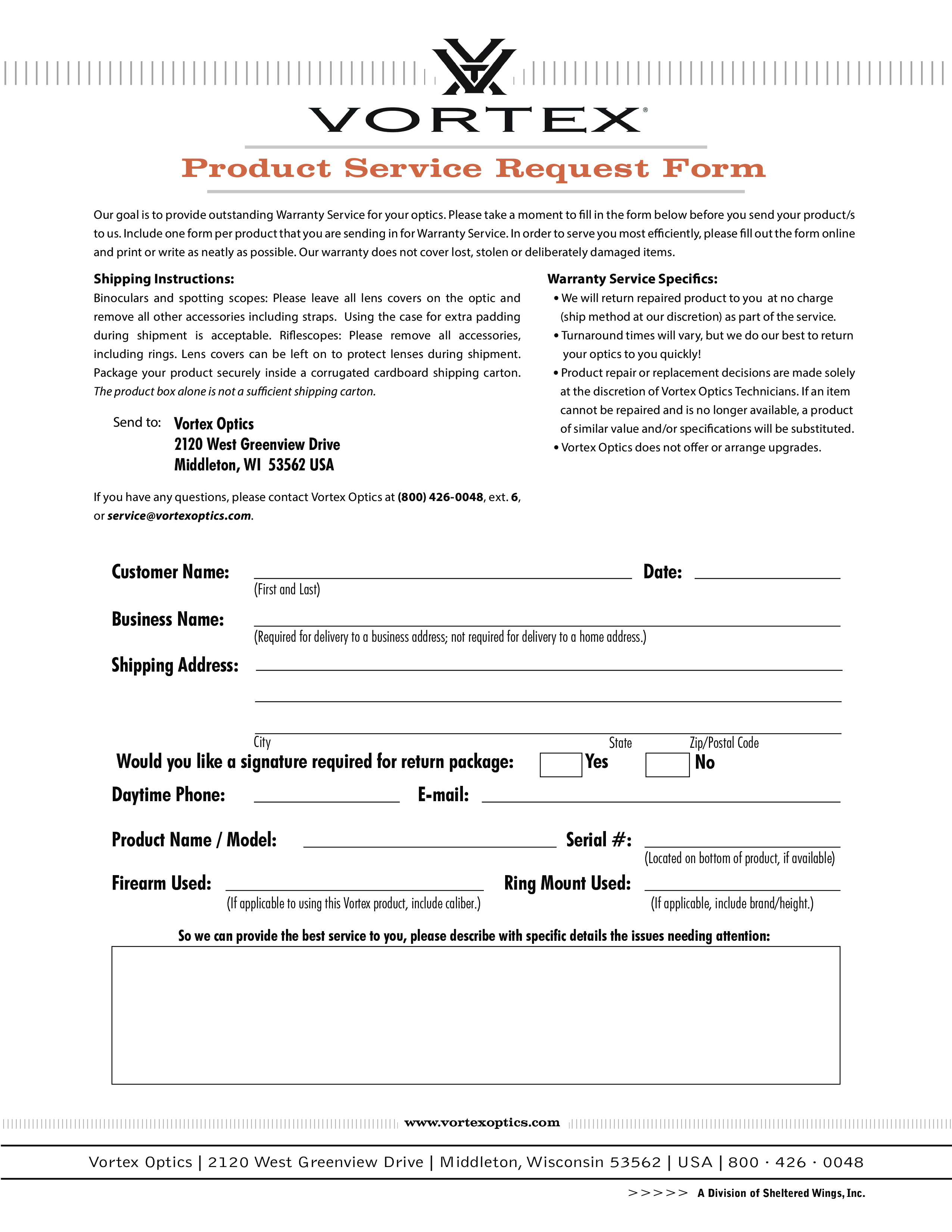
Customer Name: Business Name: Date: (First and Last) (Required for delivery to a business address not required for delivery to a home address.) Shipping Address: City Would you like a signature required for return package: Daytime Phone: State Zip/Postal Code No E-mail: Product Name / Model: Firearm Used: Yes Serial : (If applicable to using this Vortex product, include caliber.) Ring Mount Used: (Located on bottom of product, if available) (If applicable, include brand/height.) So we can provide the best service to you, please describe with specific details the issues needing attention: www.vortexoptics.com Vortex Optics 2120 West Greenview Drive Middleton, Wisconsin 53562 USA 800 · 426 · 0048 A Division of Sheltered Wings, Inc..
DISCLAIMER
Nothing on this site shall be considered legal advice and no attorney-client relationship is established.
Leave a Reply. If you have any questions or remarks, feel free to post them below.
Related templates
Latest templates
Latest topics
- GDPR Compliance Templates
What do you need to become GDPR compliant? Are you looking for useful GDPR document templates to make you compliant? All these compliance documents will be available to download instantly... - Google Docs Templates
How to create documents in Google Docs? We provide Google Docs compatible template and these are the reasons why it's useful to work with Google Docs... - IT Security Standards Kit
What are IT Security Standards? Check out our collection of this newly updated IT Security Kit Standard templates, including policies, controls, processes, checklists, procedures and other documents. - Letter Format
How to format a letter? Here is a brief overview of common letter formats and templates in USA and UK and get inspirited immediately! - Google Sheets Templates
How to work with Google Sheets templates? Where to download useful Google Sheets templates? Check out our samples here.
cheese