Patient Registration Form
Save, fill-In The Blanks, Print, Done!

Download Patient Registration Form
Microsoft Word (.docx)Or select the format you want and we convert it for you for free:
- This Document Has Been Certified by a Professional
- 100% customizable
- This is a digital download (20.42 kB)
- Language: English
- We recommend downloading this file onto your computer.

How to create a Patient Registration Form? Are you looking for a Patient Registration Form to register incoming patients for your clinic or hospital? Download this Patient Registration Form template that will perfectly suit your needs.
When you need a patient registration form, make sure it's connected to all the relevant processes. The goal of this kind of form is to make note of all the incoming patient information, so you will have a seamless billing process. To make it easier for the patients, make sure all the relevant information is known and complete on the day of the take in. If the information is related to a minor, ask the relevant information of the patient from their parent or guardian during the registration process.
Medical information patient registration:
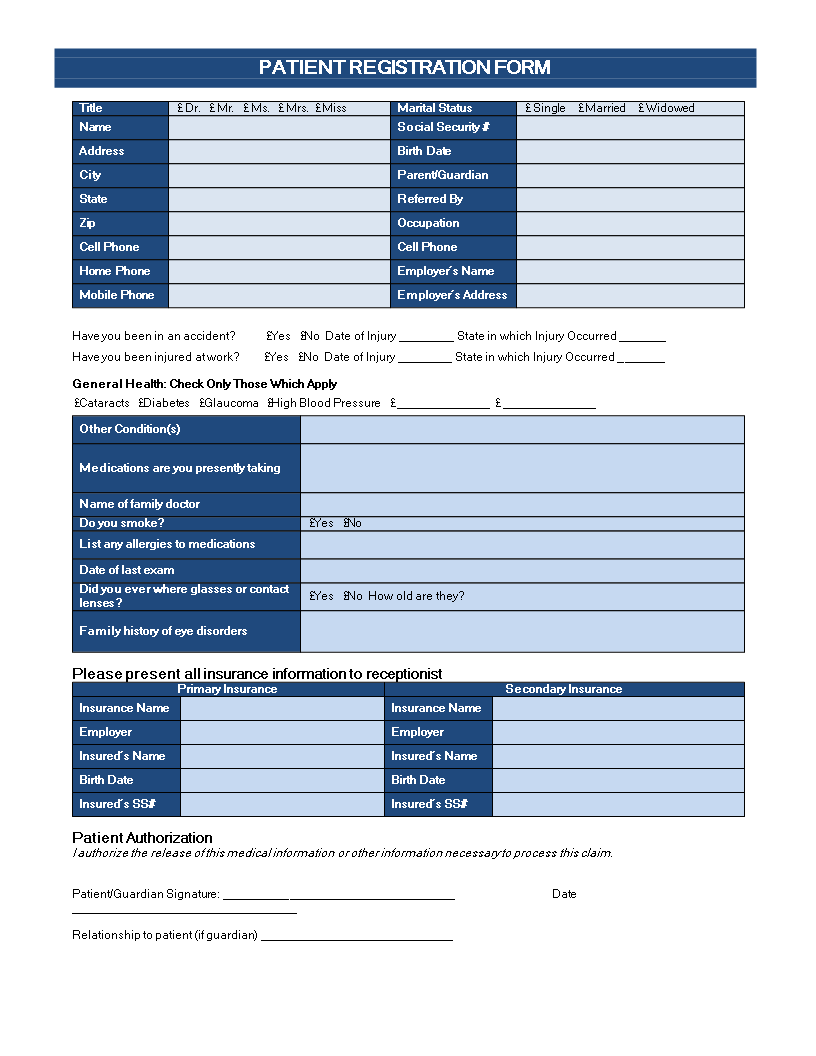
Mrs. Miss Marital Status Single Married Widowed Name Social Security Address Birth Date City Parent/Guardian State Referred By Zip Occupation Cell Phone Cell Phone Home Phone Employer s Name Mobile Phone Employer s Address Have you been in an accident Yes No Date of Injury ________ State in which Injury Occurred _______ Have you been injured at work Yes No Date of Injury ________ State in which Injury Occurred _______ General Health: Check Only Those Which Apply Cataracts Diabetes Glaucoma High Blood Pressure ______________ ______________ Other Condition(s) Medications are you presently taking Name of family doctor Do you smoke Yes No List any allergies to medications Date of last exam Did you ever where glasses or contact lenses Yes No How old are they Family history of eye disorders Please present all insurance information to receptionist Primary Insurance Secondary Insurance Insurance Name Insurance Name Employer Employer Insured s Name Insured s Name Birth Date Birth Date Insured s SS Insured s SS Patient Authorization I authorize the release of this medical information or other information necessary to process this claim..
Our collection of online healthcare templates aims to make life easier for you. By providing you this health Patient Registration template, we hope you can save precious time, cost and effort and it will help you to reach the next level of success in your life, studies or work! This blank Patient Registration Form is intuitive, ready-to-use and structured in a smart way. Try it now and let this template inspire you. Download this Registration Form for medical information now!
Also interested in other health and healthcare templates? Just search on our search bar or browse through our thousands of free and premium health forms and templates, contract, documents, letters, etc., which are used by professionals in the healthcare industry.
For example: health care directive, mental health treatment plan, health management report, allergy log, healthy weekly meal plans, sick leave letter, health evaluation form, and much more. All business templates are easy and quick to find, crafted by professionals, easy-to-customize, wisely structured, ready-made and intuitive. Pay close attention to the several options available for you by browsing through the list of health related templates. Take the time to review and choose the variety of healthcare templates to suit your need.
DISCLAIMER
Nothing on this site shall be considered legal advice and no attorney-client relationship is established.
Leave a Reply. If you have any questions or remarks, feel free to post them below.
Related templates



Latest templates
Latest topics
- GDPR Compliance Templates
What do you need to become GDPR compliant? Are you looking for useful GDPR document templates to make you compliant? All these compliance documents will be available to download instantly... - Google Docs Templates
How to create documents in Google Docs? We provide Google Docs compatible template and these are the reasons why it's useful to work with Google Docs... - IT Security Standards Kit
What are IT Security Standards? Check out our collection of this newly updated IT Security Kit Standard templates, including policies, controls, processes, checklists, procedures and other documents. - Letter Format
How to format a letter? Here is a brief overview of common letter formats and templates in USA and UK and get inspirited immediately! - Google Sheets Templates
How to work with Google Sheets templates? Where to download useful Google Sheets templates? Check out our samples here.
cheese