HTML Preview Diabetes Care Note page number 1.
___________________________________________________________________________________________________
___________________________________________________________________________________________________
—
Diabetes care patient notes: Part 1
Use the form below to track and assess patient progress. You may wish to retain
this form in the progress notes section of the patient's medical chart.
Patient name: _____________________________________________________
Vital Signs
Date: ____________________ Medical Record #: ______________________
□
Male
□
Female
Tobacco use:
□
Yes
□
No A1C:_______mg/dL
WT: __________ RR: ___________
Preprandial glucose:_______mg/dL
HT: __________ BP: ___________
Lipid: Total______mg/dL LDL______ HDL ______ Triglycerides_______
HR: __________ Temp: _________
Medications: _________________________________________________________________________________________
Head and neck: ___________________________________________
Lungs: ___________________________________________________
Heart: ___________________________________________________
Abdomen: ________________________________________________
Extremities: ______________________________________________
Neuro: __________________________________________________
Other (e.g., eye, dental): _____________________________________
________________________________________________________________________________________________
Physical Exam
Patient assessment follow up as necessary (Check best answer)
Have you visited an emergency room or urgent care office or been admitted to the hospital for
treatment of diabetes problems since your last visit?
□
No
□
Yes
How many times a day do you test your blood sugar with your meter?
□
1
□
2 or more
Do you have any trouble telling when you have low blood sugar?
□
No
□
Yes
How many times per week do you have low blood sugar during the day?
□
0
□
1 or more
How many times per week do you have low blood sugar at night?
□
0
□
1 or more
Do you have any problems with your medicines?
□
No
□
Yes
Have you noticed any problems with your eyes, feet, or skin since your last visit?
□
No
□
Yes
Other: ____________________________________________________________________________________________
Do you ever have:
□
Chest pain
□
Claudication
□
Foot ulcers/rashes
□
Urinary tract symptoms
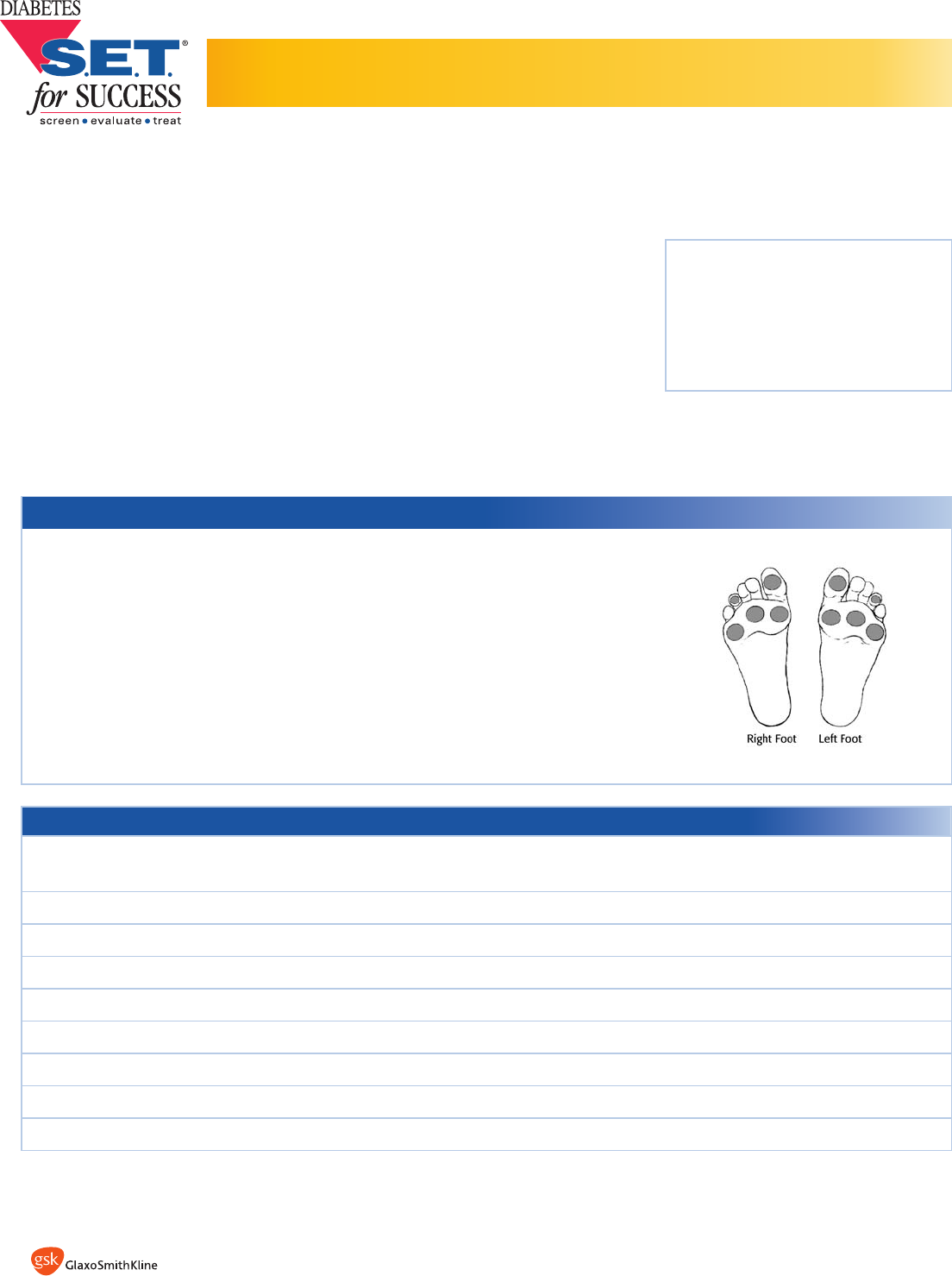
Foot Exam Test Areas
Indicate
Presence (+)
or Absence (-)
of sensation in
5 areas using
10-gram
monofilament
This material has been developed by GlaxoSmithKline.
©2006 The GlaxoSmithKline Group of Companies All rights reserved. Printed in USA. MM1310R0 March 2006
Diabetes S.E.T. for Success is a registered trademark of the GlaxoSmithKline Group of Companies.