HTML Preview Overtime Compensatory Time Authorization Form page number 1.
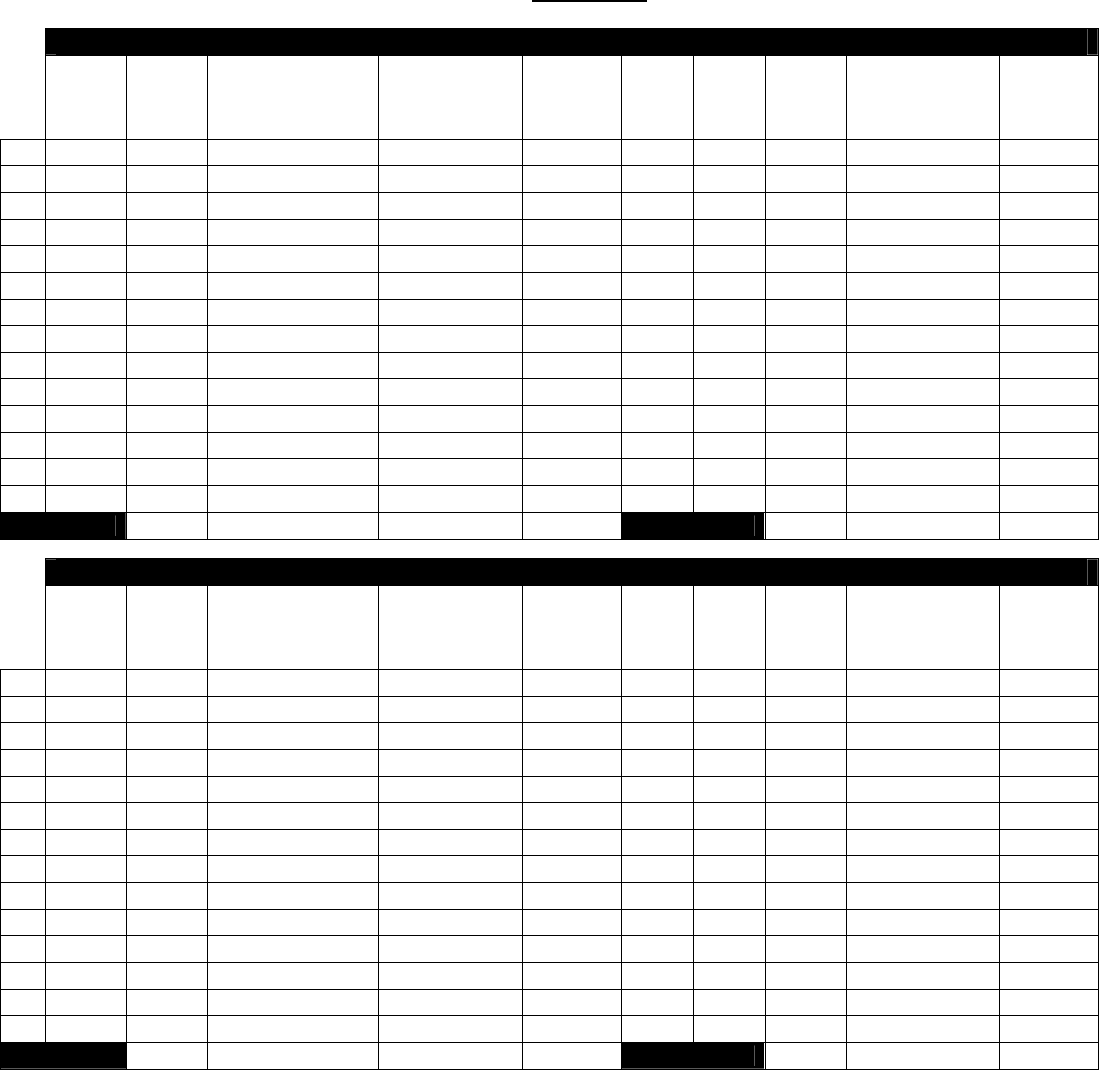
OVERTIME/COMPENSATORYTIMEAUTHORIZATIONFORM
EmployeeName:__________________________________________________ ____ Personnel#:_______________________
OrgUnitName/#:_______________________________________________PayPeriodStart/EndDate:___________________
OVERTIMEAPPROVAL
Date
Est.#
Hours
ToBe
Worked
Reasonfor
Overtime
Request
OVERTIME
PRE‐APPROVED
BY
DATE
Estimated
Hours
Approved
Actual
Time
In
Actual
Time
Out
Actual#
of
Hours
Worked
ACTUAL
OVERTIME
APPROVEDBY
DATE
Actual
Hours
Approved
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
TotalEst.Hrs.
TotalActualHrs.
COMPENSATORY TIME APPROVAL
Date
Est.#
Hours
ToBe
Worked
Reasonfor
CompensatoryTime
Request
COMPENSATORY
TIME
PRE‐APPROVED
BY
DATE
Estimated
Hours
Approved
Actual
Time
In
Actual
Time
Out
Actual#
of
Hours
Worked
ACTUAL
COMPENSATORY
TIME
APPROVEDBY
DATE
Actual
Hours
Approved
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
TotalEst.Hrs.
TotalActualHrs.
PerBoardPolicy,allOvertimeandCompensatorytime MUSTBEPRE‐APPROVED.Fillin theestimatednumberofhoursandthe reasonforovertime/comp
timebydayintheappropriateOvertime/CompensatoryTimesection.Eachdatetobeworkedshouldbeenteredseparately.Thesupervisormustsignbelow
and in the
Approved By column for each date.After working overtime or comp time, record the actual time in and out, and the actual number of hours
workedeachdaytothenearestquarterhour(.00,.25,.50,.75)attheSTRAIGHTTIMErate.ThesupervisormustsignintheApprovedBycolumn
foreachdate
actuallyworked.(NOTE:anOvertime/CompensatoryTimeAuthorizationformshouldbefilledoutforeachpayperiodwhenovertimeorcompensatorytime
mayberequired.AVacationLeaveRequestformshouldbecompletedwhencompensatorytimeisused.)
_____________________________________________________________ ___________________________________________
EmployeeSignatureDate
_______________________________________________________________________________________________________
SupervisorName(PleasePrint) SupervisorSignatureDate
Form#4707Revised7.21.2011