HTML Preview Application Form For Insurance page number 1.
NAME AND MAILING ADDRESS OF 2ND MORTGAGEE LOSS PAYEE OTHER
IF OTHER, SPECIF Y:
/
/
/ /
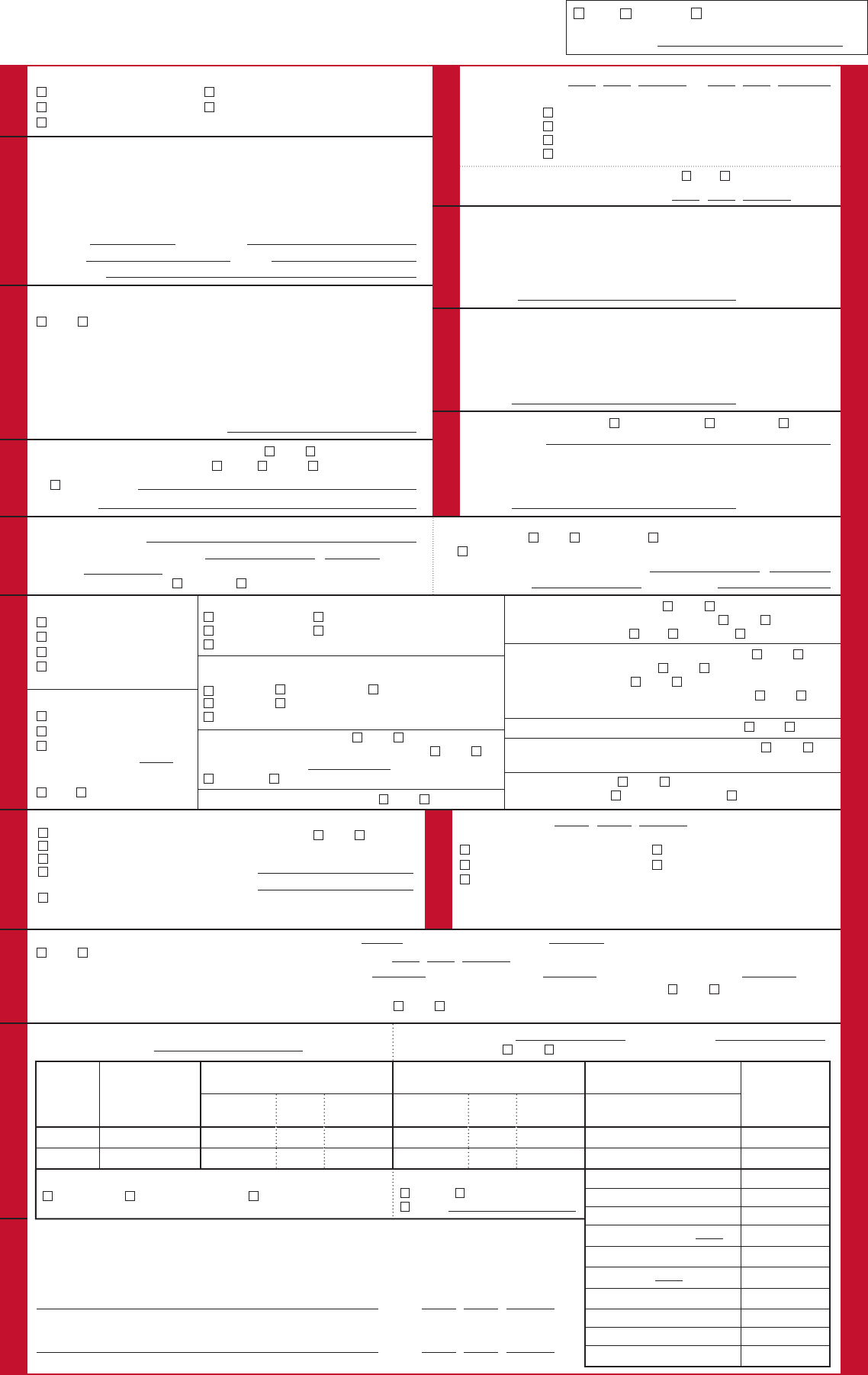
U.S. DEPARTMENT OF HOMELAND SECURITY
FEDERAL EMERGENCY MANAGEMENT AGENCY
National Flood Insurance Program
FLOOD INSURANCE APPLICATION, PART 1 (OF 2)
IMPORTANT—PLEASE PRINT OR TYPE; ENTER DATES AS MM/DD/YYYY.
O.M.B. No. 1660-0006 Expires November 30, 2016
NAME AND MAILING ADDRESS OF INSURED:
N
O
D
I
E
T
R
MA
SU
R
N
O
I
FNI
IS INSURANCE REQUIRED FOR DISASTER ASSISTANCE? YES NO
IF YES, CHECK THE GOVERNMENT AGENCY: SBA FEMA FHA
OTHER (SPECIF Y):
CASE FILE NO.:
NAME AND MAILING ADDRESS OF FIRST MORTGAGEE:
NOTE: ONE BUILDING PER POLICY — BLANKET COVERAGE NOT PERMITTED.
DRESS?
ER LEGAL DESCRIPTION, OR
IS INSURED PROPERTY LOCATION SAME AS INSURED’S MAILING AD
YES NO
IF NO, ENTER PROPERTY ADDRESS. IF RURAL, ENT
PROPERTY (DO NOT USE P.O. BOX).GEOGRAPHIC LOCATION OF
Y
NEW RENEWAL TRANSFER (NFIP ONLY)
PRIOR POLICY #:
GNILLIB
FOR RENEWAL, BILL:
INSURED
FIRST MORTGAGEE
SECOND MORTGAGEE
/EEGA
R
G
E
TR
TH
OD M
O
N2
/ /
/ /
E
R
C
ET
AN
S
T
SA
S
I
SI
D
SA
YTUNIMMOC
NOITACO LYTRPEOPR
GRANDFATHERING INFORMATION
GRANDFATHERED?
YES NO IF YES, BUILT IN COMPLIANCE OR
CONTINUOUS COVERAGE (PROVIDE PRIOR POLICY NUMBER IN BOX ABOVE)
CURRENT COMMUNITY NO./PANEL NO. AND SUFFIX:
–
CURRENT FIRM ZONE:
CURRENT BFE:
FOR AN ADDRESS WITH MULTIPLE BUILDINGS AND/OR FOR A BUILDING WITH ADDITIONS OR
EXTENSIONS, DESCRIBE THE INSURED BUILDING:
PHONE NO.:
/
/
F
/
/
BUILDING DIAGRAM NO.:
/
/
LOWEST FLOOR ELEVATION:
RATING MAP INFORMATION
NAME OF COUNTY/PARISH:
COMMUNITY NO./PANEL NO. AND SUFFIX:
–
FIRM ZONE:
COMMUNITY PROGRAM TYPE IS: REGULAR EMERGENCY
EE
1ST
AGGTROM
LOSS PAYEE
OTHER (AS SPECIFIED IN THE “2ND
MORTGAGEE/
OTHER” BOX BELOW)
AGENCY NO.: AGENT’S TAX ID:
PHONE NO.: FAX NO.:
EMAIL ADDRESS:
LOAN NO.:
LOAN NO.:
N
F
I
P
C
O
P
Y
FEMA Form 086-0-1 Previously FEMA Form 81-16 F-050 (DEC 2013)
DORIE PYICLOP
POLICY PERIOD IS FROM
12:01 A.M. LOCAL TIME AT THE INSURED PROPERTY LOCATION.
WAITING PERIOD:
STANDARD 30-DAY
REQUIRED FOR LOAN TRANSACTION — NO WAITING PERIOD
MAP REVISION (ZONE CHANGE FROM NON-SFHA TO SFHA) — 1 DAY
TRANSFER (NFIP ONLY) — NO WAITING PERIOD
TO
YES NO
IF YES, INDICATE THE PROPERT Y P
URCHASE DATE:
PROPERTY PURCHASED ON OR AFTER 07/06/2012:
REC
N
U
O
D
IT
RO
MA
P
R
/T
O
N
F
E
N
G
I
A
NAME AND MAILING ADDRESS OF AGENT/PRODUCER:
LDINGUIB
BUILDING OCCUPANCY
SINGLE FAMILY
2–4 FAMILY
OTHER RESIDENTIAL
NON-RESIDENTIAL (INCLUDING
HOTEL/MOTEL)
B
UILDING PURPOSE
100% RESIDENTIAL
100% NON-RESIDENTIAL
M
IXED-USE — SPECIFY PERCENTAGE
OF RESIDENTIAL USE: %
IS BUILDING A BUSINESS PROPERTY?
YES NO
BASEMENT, ENCLOSURE, CRAWLSPACE
NONE
FINISHED BASEMENT/E
NCLOSURE
CRAWLSPACE UNFINISHED BASEMENT/ENCLOSURE
SUBGRADE CRAWLSPACE
NUMBER OF FLOORS IN BUILDING (INCLUDING BASEMENT/
ENCLOSED AREA, IF ANY) OR BUILDING T YPE
1 2 3 OR MORE
SPLIT LEVEL TOWNHO
USE/ROWHOUSE (RCBAP LOW-RISE ONLY)
MANUFACTURED (MOBILE) HOME/TRAVEL TRAILER ON FOUNDATION
IS COVERAGE FOR A CONDO UNIT? YES NO
IS BUILDING IN A CONDOMINIUM FORM OF OWNERSHIP? ES NO
TOTAL NUMBER OF UNITS:
HIGH-RISE LOW-RISE
IS BUILDING LOCATED ON FEDER
AL LAND? YES NO
IS BUILDING WALLED AND ROOFED? YES NO
I
S BUILDING IN THE COURSE OF CONSTRUCTION? YES NO
IS BUILDING OVER WATER? NO PARTIALLY ENTIRELY
IS BUILDING INSURED’S PRINCIPAL/PRIMARY RESIDENCE?
YES NO
IS BUILDING A RENTAL PROPERTY? YES NO
IS THE INSURED A TENANT? YES NO
IF YES, IS THE TENANT REQUESTING BUILDING COVERAGE? YES NO
IF YES, SEE NOTICE BELOW.
IS THE BUILDING A SEVERE R
EPETITIVE LOSS PROPERTY? YES NO
DOES THE BUILDING HAVE ANY ADDITIONS OR EXTENSIONS? YES NO
(ADDITIONS AND EXTENSIONS MAY BE SEPARATELY INSURED.)
IS BUILDING ELEVATED? YES NO
IF YES, AREA BELOW IS: FREE OF OBSTRUCTION WITH OBSTRUCTION
SNTNTEOC
CONTENTS LOCATED IN*:
BASEMENT/ENCLOSURE
BASEMENT/ENCLOSURE AND ABOVE
LOWEST FLOOR ONLY ABOVE GROUND LEVEL
LOWEST FLOOR ABOVE GROUND LEVEL
AND HIGHER
ABOVE GROUND LEVEL MORE THAN
1 FULL FLOOR
IS PERSONAL PROPERTY HOUSEHOLD
CONTENTS? YES NO
IF NO, DESCRIBE:
*IF SINGLE FAMILY, CONTENTS ARE RATED
THROUGHOUT THE BUILDING.
N
N
OI
O
T
I
C
T
UR
MA
T
R
S
O
N
F
CO
NI
CONSTRUCTION DATE:
CHECK ONE OF THE FOLLOWING:
BUILDING PERMIT
CONSTRUCTION
FOR MANUFACTURED (MOBILE) HOMES/
TRAVEL TRAILERS LOCATED OUTSIDE A
MOBILE HOME PARK OR SUBDIVISION:
DATE OF PERMANENT PLACEMENT
SUBSTANTIAL IMPROVEMENT
OR MANUFACTURED (MOBILE) HOMES/
TRAVEL TRAILERS LOCATED IN A
MOBILE HOME PARK OR SUBDIVISION:
CONSTRUCTION DATE OF MOBILE HOME
PARK OR SUBDIVISION FACILITIES
NIOT
TA
AEV
AD
LE
IS BUILDING POST-FIRM CONSTRUCTION?
YES NO
(IF POST-FIRM CONSTRUCTION IN ZONES A,
A1–A30, AE, AO, AH, V, V1–V30, VE, OR IF PRE-
FIRM CONSTRUCTION IS ELEVATION RATED,
ATTACH ELEVATION CERTIFICATE.)
LOWEST ADJACENT GRADE (LAG):
ELEVATION CERTIFICATION DATE:
(=) DIFFERENCE TO NEAREST FOOT:
(+ OR –)
IN ZONES V AND V1–V30 ONLY, DOES BASE FLOOD ELEVATION INCLUDE EFFECTS OF WAVE ACTION? YES NO
IS BUILDING FLOODPROOFED? YES NO (SEE THE NFIP FLOOD INSURANCE MANUAL FOR CERTIFICATION FORM.)
(
–) BASE FLOOD ELEVATION:
GNIT RADN AGERAEVOC
ESTIMATED BUILDING REPLACEMENT COST
(INCLUDING FOUNDATION): $
DEDUCTIBLE: BUILDING $
DEDU
CTIBLE BUYBACK? YES NO
CONTENTS $
INSURANCE
COVERAGE
TOTAL AMOUNT AMOUNT OF
OF INSURANCE INSURANCE
BASIC LIMITS
RATE
ANNUAL
PREMIUM
ADDI
(REGULA
AMOUNT OF
INSURANCE
TIONAL LIMI
R PROGRAM
RATE
TS
ONLY)
ANNUAL
PREMIUM
BUILDING .00
CONTENTS .00
RATE CATEGORY:
MANUAL SUBMIT FOR RATE PROVISIONAL RATING
.00
.00
PAYMENT METHOD:
CHECK CREDIT CARD
OTHER:
DEDUCTIBLE
TOTAL
PREMIUM REDUCTION/INCREASE PREMIUM
.00 .00
.00 .00
ANNUAL SUBTOTAL $
ICC PREMIUM
SUBTOTAL
CRS PREMIUM DISCOUNT %
SUBTOTAL
RESERVE FUND
%
SUBTOTAL
PROBATION SURCHARGE
FEDERAL POLICY FEE
TOTAL AMOUNT DUE
$
EURTANIGS
NOTICE: BUILDING COVERAGE BENEFITS — EXCEPT FOR A RESIDENTIAL CONDOMINIUM BUILDING — ARE NOT AVAILABLE IF OTHER NFIP
BUILDING COVERAGE HAS BEEN PURCHASED BY THE APPLICANT OR ANY OTHER PARTY FOR THE SAME BUILDING.
THE ABOVE STATEMENTS ARE CORRECT TO THE BEST OF MY KNOWLEDGE. I UNDERSTAND THAT ANY FALSE STATEMENTS MAY BE PUNISHABLE
BY FINE AND/OR IMPRISONMENT UNDER APPLICABLE FEDERAL LAW. SEE REVERSE SIDE OF COPIES 2, 3, AND 4.
SIGNATURE OF INSURANCE AGENT/PRODUCER DATE (MM/DD/YYYY)
SIGNATURE OF INSURED (OPTIONAL) DATE (MM/DD/YYYY)
PLEASE SUBMIT TOTAL AMOUNT DUE WITH THE NFIP COPY OF THIS APPLICATION.
IF PAYING BY CHECK OR MONEY ORDER, MAKE PAYABLE TO THE NATIONAL FLOOD INSURANCE PROGRAM.
IMPORTANT — COMPLETE PART 1 AND PART 2 (ON LAST PAGE) BEFORE SENDING APPLICATION TO THE NFIP. — IMPORTANT