HTML Preview Hospital Operating Budget page number 1.
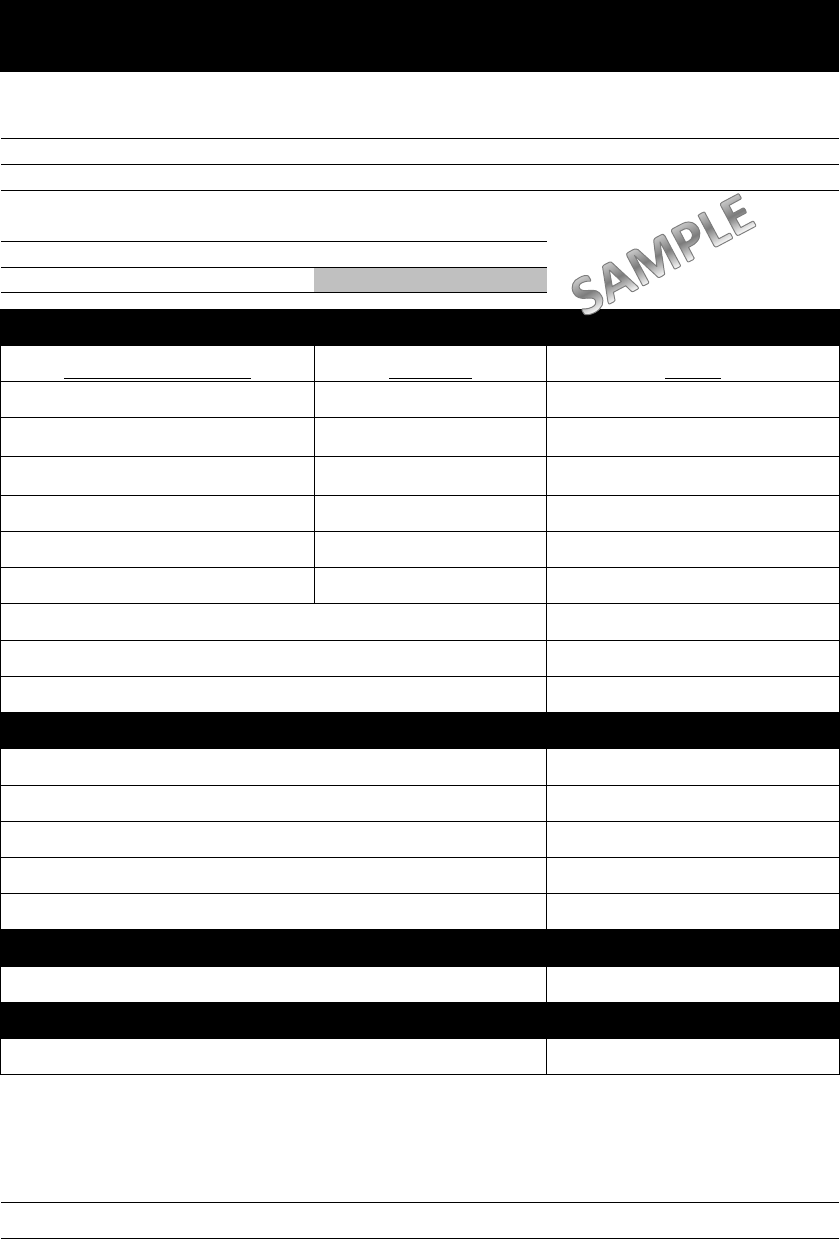
Title/Department: Director of Nursing
Phone Number: 318-999-9999
Fax Number: 318-999-9998
Reimbursable Limit: 10,000.00
Match Amount (10%): 1,000.00
TOTAL OBLIGATION AMOUNT: 11,000.00
Capability Planning Guide
Description Amount
CPG 1 - Healthcare System Preparedness Training
$ 5,000.00
CPG 2 - Recovery
HVA Assessment, Development
of SOP/COOP $ 750.00
CPG 3 - Emergency Operation Coordination
HEICS vests, Command Center
Equipment $ 450.00
CPG 5 - Mass Fatality Body Bags $ 300.00
CPG 6 - Information System 700 MHz Radio $ 1,000.00
CPG 10 - Medical Surge
B
e
d
capac
it
y equ
i
pmen
t
,
Decontamination Tent $ 2,000.00
CPG 14 - Responder Safety PPE, Pharmaceuitical Cache $ 2,000.00
CPG 15 - Volunteer Management "Just in Time" Training Modules $ 1,000.00
$ 12,500.00
$ -
$ 300.00
$ -
$ -
$ 300.00
$ 12,800.00
1,800.00$
CEO's Name (Print): Date:
CEO's Signature:
C. TOTAL AMOUNT PROPOSED (Cash Expenditures + In-Kind Contributions)
AMOUNT OVER TOTAL OBLIGATION
A. CASH EXPENDITURES
B. NON CASH IN-KIND CONTRIBUTIONS
D. OVERAGE (Total Amount Proposed - Total Obligation Amount)
Staff Time
Meeting Space
Storage/Rental Space
FY 2013-2014 Budget Proposal
Health and Human Services (HHS) Grant
TOTAL AMOUNT
By signing below, you are ensuring that HHS grant funds will be spent in accordance with the guidelines as
specified in your Participation Agreement.
Mileage Reimbursement
TOTAL NON CASH IN-KIND CONTRIBUTIONS
TOTAL CASH EXPENDITURES
Organization Name: Sunny Beach Hospital
Contact Person: John Doe
Email Address: joe.doe@hospital.com