HTML Preview Printable Patient Medication List page number 1.
3/08 med_list_form.pdf
P
P
a
a
t
t
i
i
e
e
n
n
t
t
M
M
e
e
d
d
i
i
c
c
a
a
t
t
i
i
o
o
n
n
L
L
i
i
s
s
t
t
Patient Name:
Date of Birth:
Sex: (circle one)
Male Female
Height: Weight:
Pharmacy: (Name/Telephone)
Allergies/Adverse effects to Medication:
Medical Providers:
(Name/Address/Telephone)
Immunizations: (Month/Year)
Flu Vaccine __________________
Pneumonia
__________________
Tetanus __________________
1. Complete the patient information section above (including significant allergies or adverse reactions to medications)
2. Maintain an up-to-date list of all your medications (including OTC, herbal, or natural medications; vitamins and minerals)
3. Present this list to all your providers
Name of Medicine (brand or generic) –
Dose (mg, puffs, drops) – Schedule (times per day, etc.)
Date
Started / Stopped
Reason to use medication –
Comments
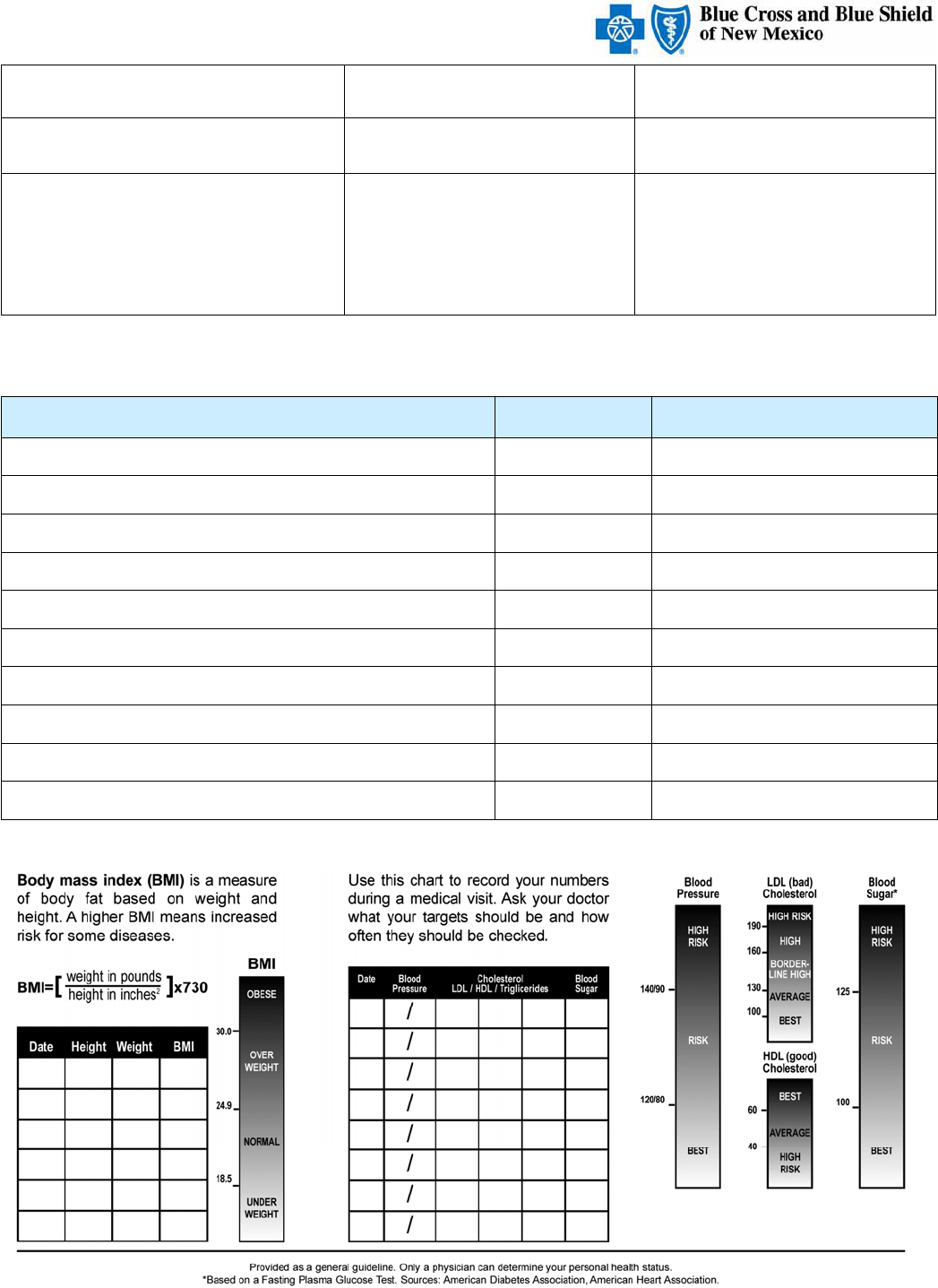
Know Your Numbers
A Division of Health Care Service Corporation, a Mutual Legal Reserve Company,
an Independent Licensee of the Blue Cross and Blue Shield Association.