HTML Preview Printable Note page number 1.
1
Skilled Nursing Note
Client Name:
PMI Patient Number: DATE(MM/DD/YYYY): TIME IN: TIME OUT:
PAIN ASSESSMENT
Is the client experiencing pain now? Yes No
If yes, answers questions below based on client’s condition
Client’s pain goal: No pain Partial relied (target score) _______________
Other ____________________________________________
Location of pain:
Observation of pain site:
Management of pain:
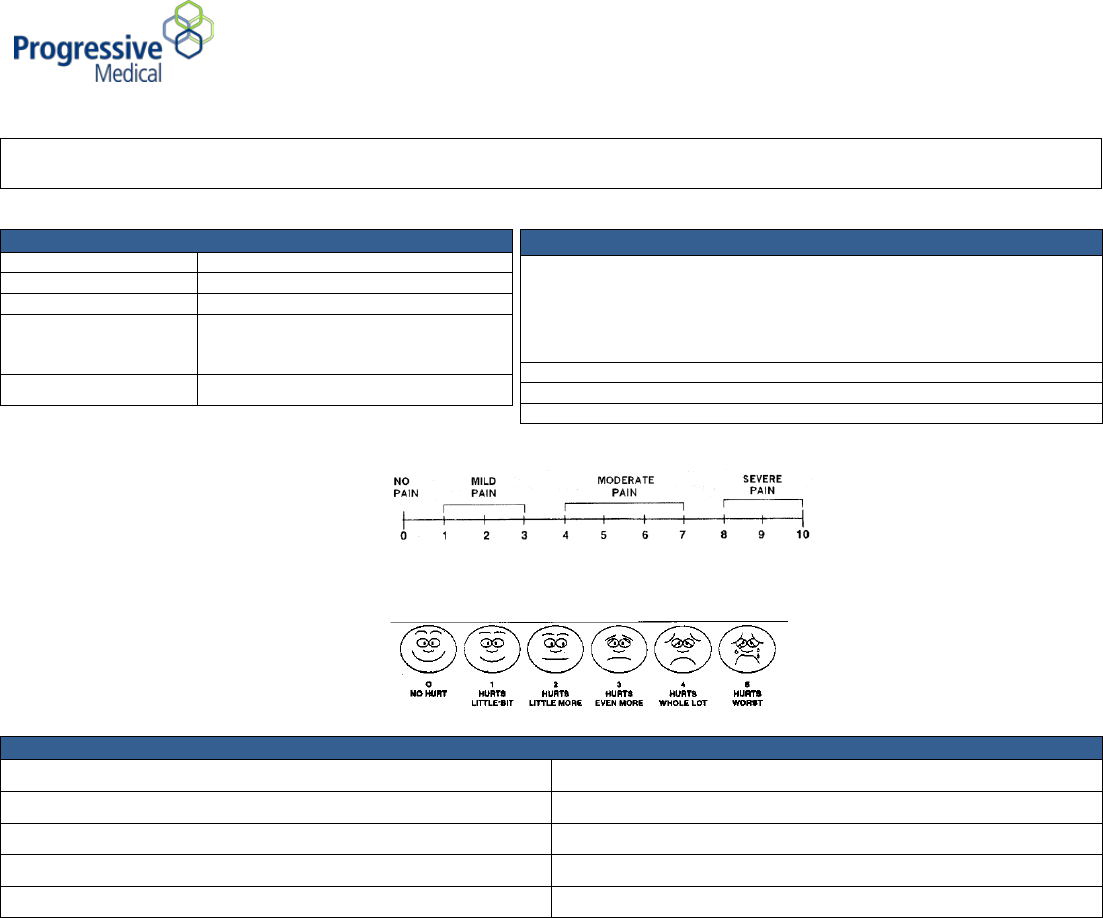
PAIN INTENSITY SCALE
WONG-BAKER FACES SCALE
ASSESSMENT
Nutrition Changes:
Respiratory:
Sensory Changes:
Environment/Safety:
Bowel:
Cardiac Status:
Urinary:
Respiratory Status:
Psycho/Neurologic:
Other:
Shift/Visit Notes: ________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________
Outcome for this shift/visit (Progress towards goals): __________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________
Instructions provided/patient education: ___________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________
_____________________________________________ ___________________________________________ ____________________
Nurse Signature and Title Print Name Date
_____________________________________________ ___________________________________________ ____________________
Client or Representative Signature Relationship Date
VITAL SIGNS
Temperature
Pulse
Respiration
Blood Pressure
________ / __________
________ / ___________
Weight/BMI
________ / ___________