HTML Preview Goods Purchase Order page number 1.
Justification Needed? (Circle one) Yes No
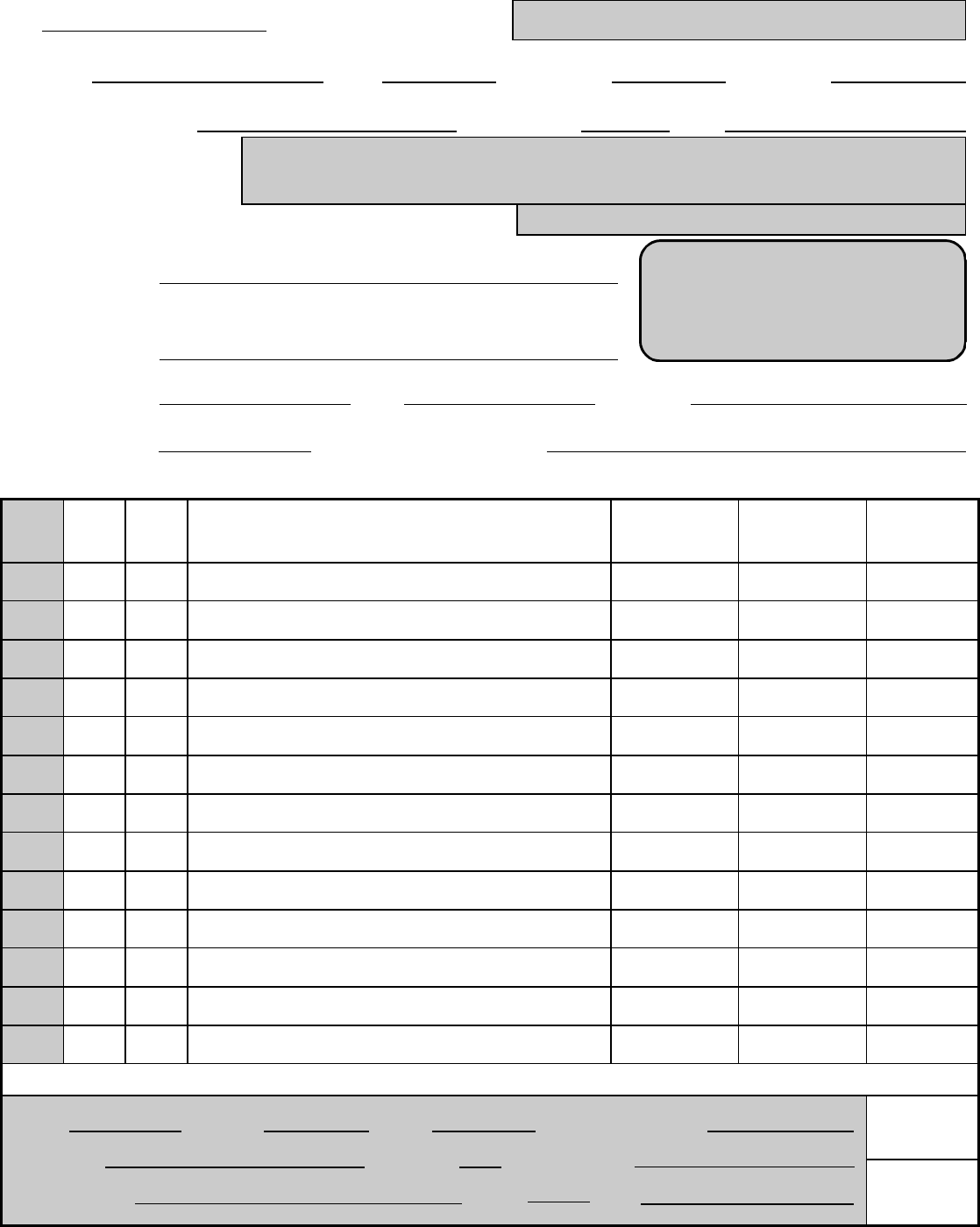
Suggested Vendor:
Address:
Phone:
Date Wanted:
Fax: Contact:
Shipping Instructions:
Purchase Order Request Form
(Shaded areas for Purchasing use only)
Date: Purchase Order Number:
Requestor: Bldg: Room No: Phone Ext:
Principal Investigator: Budget Code: Dept:
Comm
.
Codes
Qty
Unit
Of
Issue
ITEM NAME AND DESCRIPTION
(Include manufacturer, name, model or type number and any other
identifying information)
Catalog
Number
Unit Price
Total Cost
If modifying existing equipment, ADD VALUE to UCI Property Number:
F.O.B. Ship By: Terms: Delivery Location:
Spoke To: Tax Code: Delivery Date:
Vendor Ref # Buyer: Date:
Approved By: 9-
9-
**Urgent**
Packing slip must be turned in
to Purchasing, RH 162, within
3 days of receipt of order.
CHECK BOX IF THIS IS A PRECURSOR CHEMICAL
09/17/2012