Productreparatie bestelformulier 1
Opslaan, invullen, afdrukken, klaar!
De beste manier om een Productreparatie bestelformulier 1 te maken? Check direct dit professionele Productreparatie bestelformulier 1 template!
Beschikbare bestandsformaten:
.pdf- Gevalideerd door een professional
- 100% aanpasbaar
- Taal: English
- Digitale download (134.02 kB)
- Na betaling ontvangt u direct de download link
- We raden aan dit bestand op uw computer te downloaden.
formulier dienst Technologie alsjeblieft Optiek Postcode
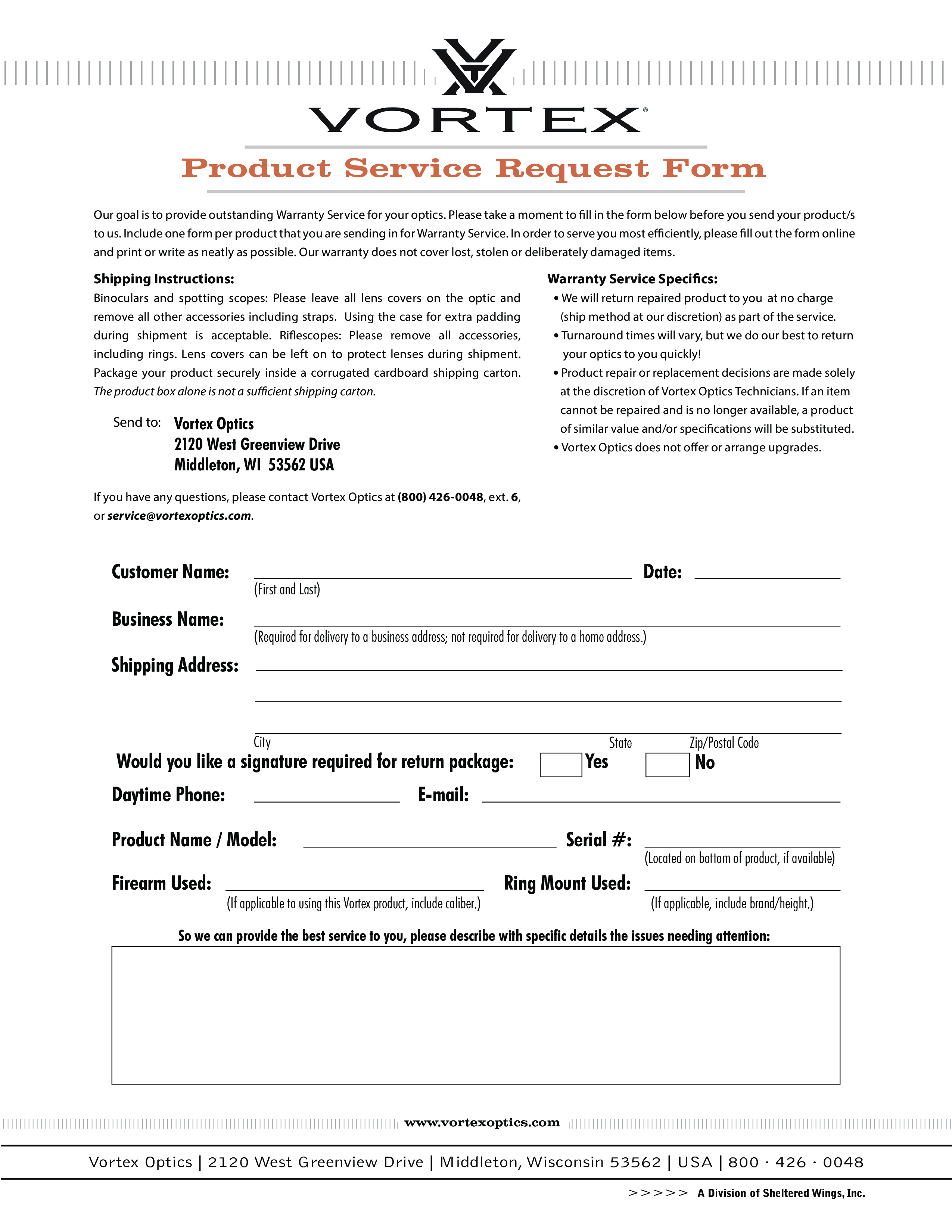
Customer Name: Business Name: Date: (First and Last) (Required for delivery to a business address not required for delivery to a home address.) Shipping Address: City Would you like a signature required for return package: Daytime Phone: State Zip/Postal Code No E-mail: Product Name / Model: Firearm Used: Yes Serial : (If applicable to using this Vortex product, include caliber.) Ring Mount Used: (Located on bottom of product, if available) (If applicable, include brand/height.) So we can provide the best service to you, please describe with specific details the issues needing attention: www.vortexoptics.com Vortex Optics 2120 West Greenview Drive Middleton, Wisconsin 53562 USA 800 · 426 · 0048 A Division of Sheltered Wings, Inc..
DISCLAIMER
Hoewel all content met de grootste zorg is gecreërd, kan niets op deze pagina direct worden aangenomen als juridisch advies, noch is er een advocaat-client relatie van toepassing.
Laat een antwoord achter. Als u nog vragen of opmerkingen hebt, kunt u deze hieronder plaatsen.