Vergoeding claimformulier

Opslaan, invullen, afdrukken, klaar!
De beste manier om een Vergoeding claimformulier te maken? Check direct dit professionele Vergoeding claimformulier template!
Beschikbare bestandsformaten:
.pdf- Gevalideerd door een professional
- 100% aanpasbaar
- Taal: English
- Digitale download (929.45 kB)
- Na betaling ontvangt u direct de download link
- We raden aan dit bestand op uw computer te downloaden.
Zakelijk verzekering vordering Naam schadeclaim verzekeringsclaim Formulieren Kilometervergoeding formulier Vergoedingsformulier Datum Onkostenvergoedingsformulier Personeelsvergoeding formulier Eenvoudige vergoedingsformulieren Vergoeding claimformulier Medewerkersvergoeding formulier eenvoudig Medewerkersvergoedingsformulier verzekeringsclaims in Verzekeringsclaim sjabloon een verzekeringsclaim verzekerings claims
How to create a Reimbursement Claim Form as Insurer? How do I fill out a reimbursement form? Are you looking for a professional Reimbursement Claim Form?
This expense reimbursement form is used to allow employees to submit their claims for reimbursement for any kind of business expenses, that will be paid by the company, while conducting business on behalf of an organization, and for petty cash replenishments. Often such expenses were paid by the employee him or herself. The responsibility for completing an accurate, compliant, and properly authorized reimbursement claims rests solely by the employee/person that prepares the form, or the account holder. Since every day brings new projects, emails, documents, and task lists, and often they go hand in hand with expenses, it's very common to work with a standard reimbursement form in your organization that everybody can fill in and file at Accounts or Finance department. This Reimbursement Claim Form template can help you find inspiration and motivation. This Reimbursement Claim Form covers the most important topics that you are looking for and will help you to structure and communicate in a professional manner with those involved.
Address Enter the full postal address Include
Street, City and Pin code
Phone No Enter the phone number of patient Include STD code with telephone number
1) E-mail ID Enter e-mail address of patient Complete e-mail address
DETAILS OF HOSPITALIZATION
a) Name of Hospital where admited Enter the name of hospital Name of hospital in full
b) Room category occupied indicate the room category occupied Tick the right option
c) Hospitalization due to indicate reason of hospitalization Tick the right option
d) Date of injury/Date Disease first detected / Date of Delivery Enter the relevant date Use dd-mm-yy format
e) Date of admission Enter date of admission Use dd-mm-yy format
f) Enter time of admission Use hh-mm- format
g) Date of discharge Enter date of discharge Use dd-mm-yy format
h) Time Enter time of discharge Use hh-mm- format
I) If injury give cause indicate cause of injury Tick the right option If Medico legal indicate whether injury is medico-legal Tick Yes or No Reported to Police indicate whether police report was filed Tick Yes or No MLC Report Police FIR attached indicate whether MLC report and Police FIR attached Tick Yes or No System of Medicine Enter the system of medicine followed in treating the patient Open Text f) j) Time
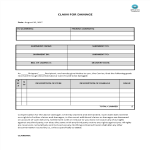
SECTION E - DETAILS OF CLAIM
a) Details of Treatment Expences Enter the amount claimed as treatment expences In rupees (Do not enter paise values) b) Claim for Domiciliary Hospitalization indicate whether claim is for domiciliary hospitalization Tick Yes or No c) Details of Lump sum/ Cash benefit claimed Enter the amount claimed as lump sum / cash benefit In rupees (Do not enter paise values) d) Claim documents Submitted-Check List indicate which supporting documents are submitted Tick the right option SECTION F - DETAILS OF BILLS ENCLOSED Indicate which bills are enclosed with the amount in rupees SECTION G - DETAILS OF PRIMARY INSURED’s BANK ACCOUNT
a) PAN Enter the permanent account number b) Account Number Enter the
Feel free to download this intuitive form template that is available in several kinds of formats, or try any other of our basic or advanced templates, forms, or documents. Don't reinvent the wheel if you need to make a reimbursement form.
Instead, check out and download this Reimbursement Claim Form template and save yourself time and effort! You will see completing your task has never been simpler!
DISCLAIMER
Hoewel all content met de grootste zorg is gecreërd, kan niets op deze pagina direct worden aangenomen als juridisch advies, noch is er een advocaat-client relatie van toepassing.
Laat een antwoord achter. Als u nog vragen of opmerkingen hebt, kunt u deze hieronder plaatsen.