Speech Therapy Progress Note template
Enregistrer, Remplir les champs vides, Imprimer, Terminer!
How do you write a speech therapy progress note? Download your free template today and take a step towards more effective and efficient patient care.
Formats de fichiers gratuits disponibles:
.docx- Ce document a été certifié par un professionnel
- 100% personnalisable
Life Privé Education Éducation speech notes template speech notes speech therapy progress notes template speech therapy soap notes template speech therapy free therapy notes template speech notes word template google doc soap note template for speech speech therapy progress note template speech progress note template speech therapy daily notes template speaking template speech therapy soap note template speech therapy notes template
How do you write a speech therapy progress note?
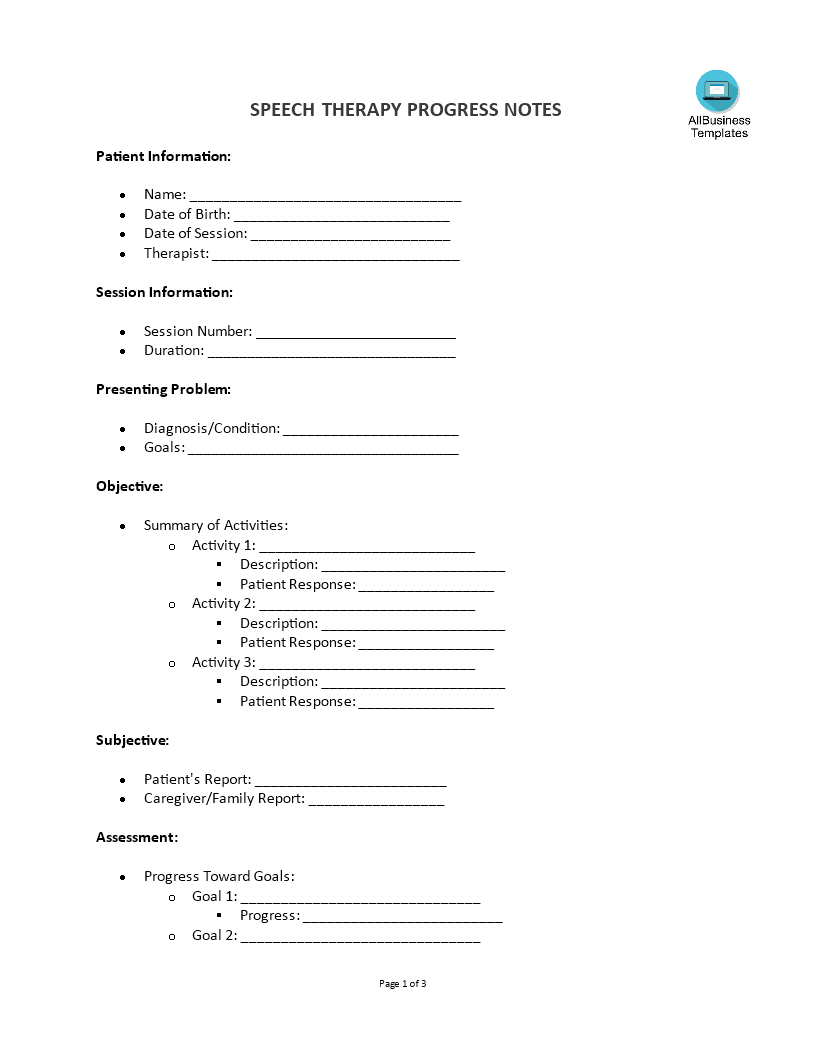
Introduction to Speech Therapy Progress Note Template
Writing a speech therapy progress note involves documenting various aspects of a therapy session to track the patient’s progress, make informed decisions about future treatment, and communicate effectively with other healthcare providers. Efficient documentation is the backbone of effective speech therapy. With our Speech Therapy Progress Note Template, you can ensure that your records are thorough, organized, and easily accessible.
Here’s a step-by-step guide on how to write a comprehensive speech therapy progress note:
Step-by-Step Guide to Writing a Speech Therapy Progress Note
1. Patient Information
- Name: Record the patient's full name.
- Date of Birth: Include the patient's date of birth.
- Date of Session: Note the date when the therapy session took place.
- Therapist Name: Include your name as the therapist.
2. Session Information
- Session Number: Indicate which session number this is (e.g., Session 3 of 10).
- Duration: Record the length of the session (e.g., 45 minutes).
3. Presenting Problem
- Diagnosis/Condition: Write the patient's primary diagnosis or condition being treated, or Expressive language delay
- Goals: List the specific therapy goals for the patient.
4. Objective Section
- Summary of Activities: Describe the activities conducted during the session. Be specific about what exercises or tasks were performed.
- Goals: Increase sentence length to 5-7 words, improve articulation of /s/ and /r/ sounds
- Patient Response: Note how the patient responded to each activity.
- Activity 1: Describe the activity and patient’s response.
- Activity 2: Describe the activity and patient’s response.
- Activity 3: Describe the activity and patient’s response.
Objective:
- Activity 1: Picture description task
- Description: John described pictures using sentences.
- Patient Response: Used 4-5 word sentences, 75% accuracy with /s/ sound.
- Activity 2: Articulation drill for /r/ sound
- Description: Practiced /r/ sound in isolation and in words.
- Patient Response: 60% accuracy in isolation, 40% in words.
- Activity 3: Storytelling activity
- Description: John told a short story using picture cues.
- Patient Response: Used varied vocabulary, 70% intelligibility.
- Subjective: Patient's Report: John said he feels he is improving and enjoys the storytelling activities.
- Caregiver/Family Report: Mother reports that John is starting to use longer sentences at home.
- Assessment:
5. Subjective Section
- Patient's Report: Summarize what the patient reports about their own progress, any difficulties they are facing, or feedback about the session.
- Caregiver/Family Report: Include any relevant observations or reports from the patient’s family or caregivers.
6. Assessment
- Progress Toward Goals: Evaluate how the patient is progressing towards the therapy goals.
- Goal 1: Describe progress and any changes.
- Goal 2: Describe progress and any changes.
- Goal 3: Describe progress and any changes.
- Current Level of Functioning: Assess the patient’s current abilities in key areas.
- Speech: Describe the current state of the patient’s speech.
- Language: Note the patient's language abilities.
- Swallowing: Record observations about swallowing if relevant.
- Cognitive-Communication: Assess cognitive-communication skills.
7. Plan
- Recommended Next Steps: Outline the next steps in the therapy plan.
- Activity 1: Specify the next activity or focus area.
- Activity 2: Specify the next activity or focus area.
- Activity 3: Specify the next activity or focus area.
- Adjustments to Therapy: Note any changes to the therapy plan based on the session.
- Homework/Practice Assignments: Detail any exercises or activities the patient should practice before the next session.
Progress Toward Goals:
- Goal 1: John is starting to increase sentence length but needs more consistency.
- Goal 2: Showing improvement with /s/ sound, needs more practice with /r/ sound.
- Current Level of Functioning:
- Speech: Moderately intelligible with familiar listeners.
- Language: Using more varied vocabulary, still working on sentence structure.
- Swallowing: Not applicable.
- Cognitive-Communication: Good attention and participation during sessions.
- Plan:
Recommended Next Steps:
- Activity 1: Continue picture description tasks, increase complexity.
- Activity 2: More articulation drills for /r/ sound, incorporate into sentences.
- Activity 3: Increase storytelling activities, focus on sentence length and clarity.
- Adjustments to Therapy: Include more visual aids to support articulation practice.
- Homework/Practice Assignments: Practice /r/ sound using provided word list, describe three pictures daily.
- Additional Notes:
- Name is showing good motivation and engagement during sessions.
- Therapist Signature:
8. Additional Notes
Include any other relevant information or observations that don’t fit into the above categories.
9. Therapist Signature and Date
- Signature: Sign the progress note.
- Date: Record the date when the note was written.
- Example of a Speech Therapy Progress Note
Features of this Speech Therapy Progress Note template:
- Patient Information: Easily record essential patient details including name, date of birth, and diagnosis.
- Session Details: Log the date, duration, and specific activities conducted during each therapy session.
- Objective and Subjective Observations: Document objective measures and subjective reports from the patient and their caregivers.
- Progress Assessment: Evaluate progress towards therapy goals with detailed assessments and notes.
- Future Planning: Outline recommended next steps, adjustments to the therapy plan, and any homework assignments for the patient.
This note template is user-friendly, customizable, and designed to meet the diverse needs of speech therapists. Whether you are a seasoned professional or a student just starting out, our progress note template can help streamline your documentation process, allowing you to focus more on providing quality care to your patients. Getting your free Speech Therapy Progress Note Template is simple. Just visit AllBusinessTemplates.com and search for the template. With a few clicks, you can download and start using this essential tool in your practice. This example provides a detailed and structured format for a speech therapy progress note, ensuring all necessary information is included for effective documentation and future planning.
In the dynamic field of speech therapy, maintaining accurate and detailed progress notes is crucial for tracking patient improvement, ensuring effective treatment, and providing clear communication between therapists, patients, and caregivers. A well-structured progress note not only documents the therapeutic journey but also facilitates continuity of care and supports evidence-based practice.
Why Speech Therapy Progress Notes are Essential?
Speech therapy progress notes are vital records that capture the therapeutic interventions, patient responses, and progress towards set goals. These notes serve multiple purposes:
- Documentation of Progress: They provide a clear record of the patient's advancements and setbacks, helping therapists adjust treatment plans as needed.
- Legal Record: Progress notes act as legal documentation of the therapy provided, which can be essential in cases of insurance claims or legal matters.
- Communication Tool: They help maintain a consistent flow of information between different healthcare providers, ensuring coordinated and comprehensive care.
- Assessment and Planning: Regularly updated notes assist in the ongoing assessment of the patient's condition and the effectiveness of the therapy, guiding future sessions.
At AllBusinessTemplates.com, we understand the importance of having reliable and easy-to-use tools for professionals. That's why we offer a comprehensive Speech Therapy Progress Note Template available for free download. Our template is designed to help speech therapists efficiently document each session, ensuring that all relevant information is captured and organized.
This introduction text highlights the importance of speech therapy progress notes and provides a clear call to action for downloading the free template from AllBusinessTemplates.com.
Download this speech therapy free therapy notes template here!
AVERTISSEMENT
Rien sur ce site ne doit être considéré comme un avis juridique et aucune relation avocat-client n'est établie.
Si vous avez des questions ou des commentaires, n'hésitez pas à les poster ci-dessous.