Sample Product Repair Order Form 1
Guardar, completar los espacios en blanco, imprimir, listo!
Sample-Product-Repair-Order-Form-Download1.pdf. Easy to download and use .pdf Technology template.
Formatos de archivo disponibles:
.pdf- Este documento ha sido certificado por un profesionall
- 100% personalizable
billing facturación form formulario service Servicio product producto Technology Tecnología Please Por favor Optics Óptica Zip Code Código postal
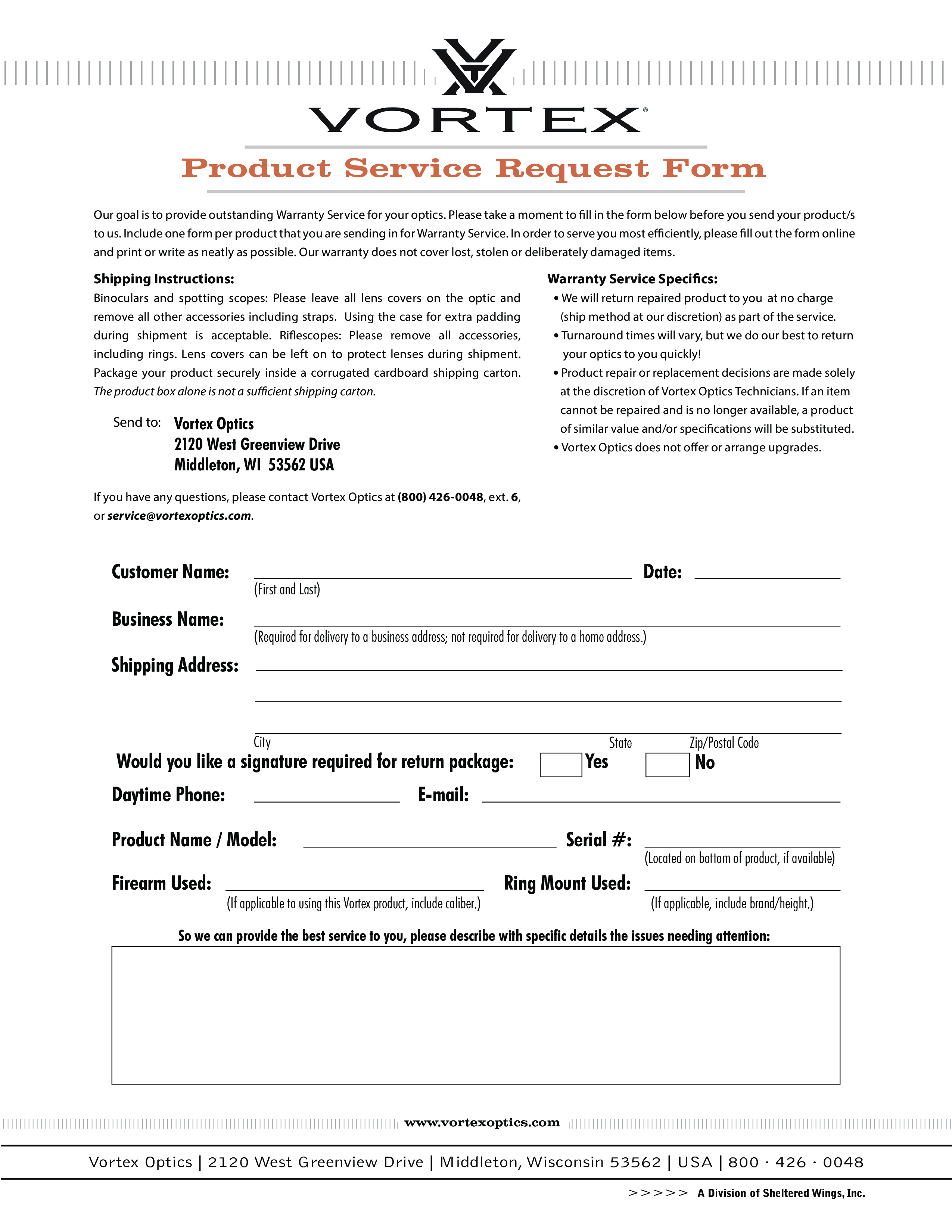
Customer Name: Business Name: Date: (First and Last) (Required for delivery to a business address not required for delivery to a home address.) Shipping Address: City Would you like a signature required for return package: Daytime Phone: State Zip/Postal Code No E-mail: Product Name / Model: Firearm Used: Yes Serial : (If applicable to using this Vortex product, include caliber.) Ring Mount Used: (Located on bottom of product, if available) (If applicable, include brand/height.) So we can provide the best service to you, please describe with specific details the issues needing attention: www.vortexoptics.com Vortex Optics 2120 West Greenview Drive Middleton, Wisconsin 53562 USA 800 · 426 · 0048 A Division of Sheltered Wings, Inc..
DESCARGO DE RESPONSABILIDAD
Nada en este sitio se considerará asesoramiento legal y no se establece una relación abogado-cliente.
Deja una respuesta. Si tiene preguntas o comentarios, puede colocarlos a continuación.