Printable Patient Sign In Sheet
Sponsored Link免费模板 保存,填空,打印,三步搞定!

Download Printable Patient Sign In Sheet
Adobe PDF (.pdf)- 本文档已通过专业认证
- 100%可定制
- 这是一个数字下载 (204.37 kB)
- 语: English
Sponsored Link
Are you looking for a professional Printable Patient Sign In Sheet? If you've been feeling stuck or lack motivation, download this template now!
Do you have an idea of what you want to draft, but you cannot find the exact words yet to write it down or lack the inspiration how to make it? If you've been feeling stuck, this Printable Patient Sign In Sheet template can help you find inspiration and motivation. This Printable Patient Sign In Sheet covers the most important topics that you are looking for and will help you to structure and communicate in a professional manner with those involved.
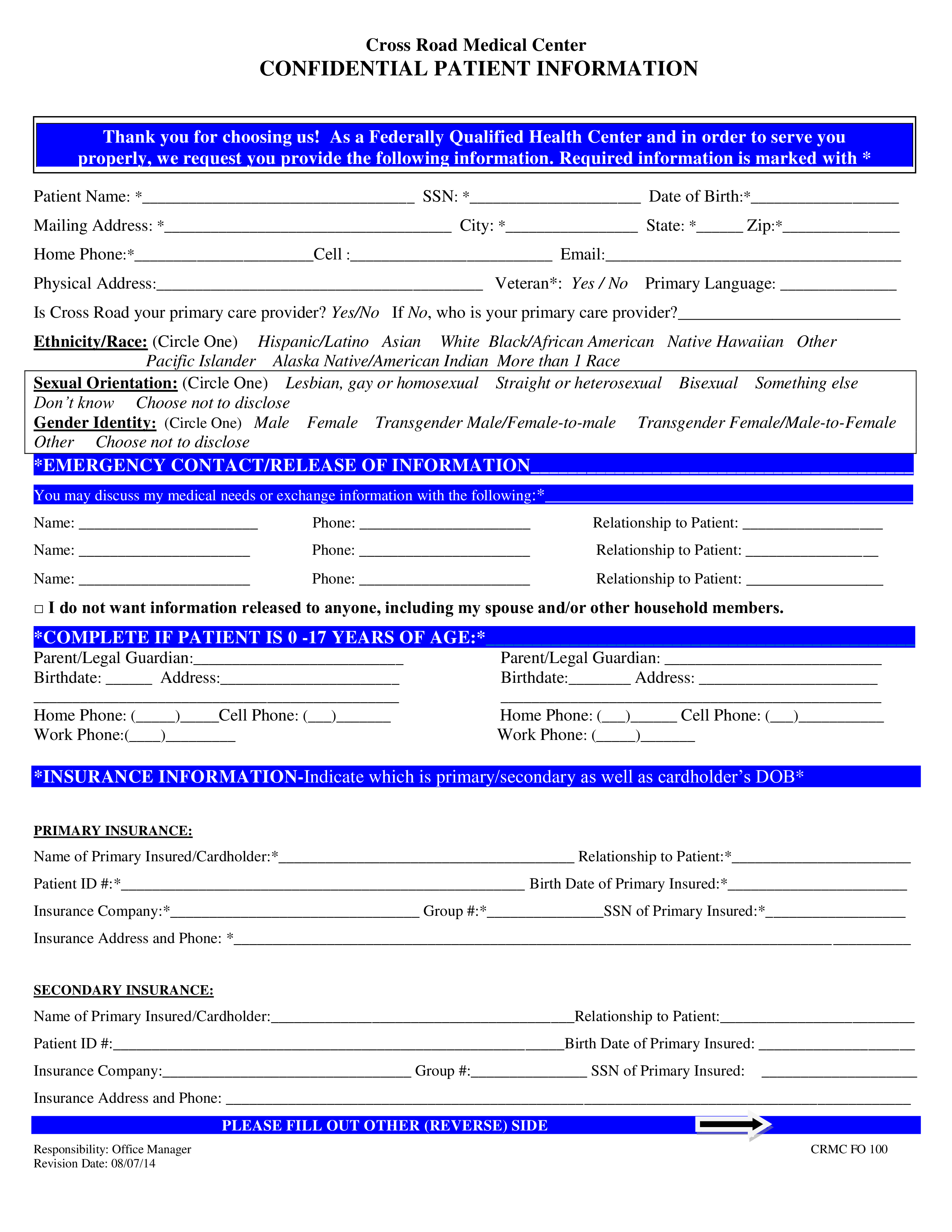
COMPLETE IF PATIENT IS 0 -17 YEARS OF AGE: Parent/Legal Guardian: Birthdate: Address: Parent/Legal Guardian: Birthdate: Address: Home Phone: ()Cell Phone: () Work Phone:() Home Phone: () Cell Phone: () Work Phone: () INSURANCE INFORMATION-Indicate which is primary/secondary as well as cardholder’s DOB PRIMARY INSURANCE: Name of Primary Insured/Cardholder: Relationship to Patient: Patient ID : Birth Date of Primary Insured: Insurance Company: Group : SSN of Primary Insured: Insurance Address and Phone: SECONDARY INSURANCE: Name of Primary Insured/Cardholder:Relationship to Patient: Patient ID :Birth Date of Primary Insured: Insurance Company: Group : SSN of Primary Insured: Insurance Address and Phone: PLEASE FILL OUT OTHER (REVERSE) SIDE Responsibility: Office Manager Revision Date: 08/07/14 CRMC FO 100
Cross Road Medical Center CONFIDENTIAL PATIENT INFORMATION EMPLOYMENT/STUDENT INFO (optional) Occupation: (Indicate if Student) Seasonal Worker: Yes/No Employer/School Name: Wor
Feel free to download this intuitive template that is available in several kinds of formats, or try any other of our basic or advanced templates, forms or documents. Don't reinvent the wheel every time you start something new...
Download this Printable Patient Sign In Sheet template and save yourself time and efforts! You will see completing your task has never been simpler!
DISCLAIMER
Nothing on this site shall be considered legal advice and no attorney-client relationship is established.
发表评论。 如果您有任何问题或意见,请随时在下面发布
相关文件
Sponsored Link